
Rampant Reflexes: Spasticity Explained
Apr 15, 2026If you live with a neurological condition — like following a stroke, a spinal cord injury, or with a disease like MS — you've likely been told at some point that your muscles are "tight" or "stiff." Maybe a well-meaning friend compared it to post-exercise soreness, or a clinician used the word spasticity without quite explaining what it means.
Spasticity is one of the most common and most misunderstood neurological symptoms. It's also one of the most important to understand, because knowing what's actually happening in your body changes how you approach it.
This post breaks down the mechanism behind spasticity, the different ways it shows up, and why managing it consistently (and early) is so important.
This article is a companion to our PK Explains video on the same topic. If you prefer to watch rather than read, check out the full episode on YouTube!
It Isn't Just Stiffness
Let's start by explaining what spasticity isn't.
Muscle stiffness after a long day at a desk isn't spasticity. Soreness after exercise isn't spasticity. Even a cramp — that sudden, involuntary, often painful contraction you sometimes get during intense activity — isn't spasticity.
And while conditions like Parkinson's disease can also cause neurological stiffness, that stiffness (called rigidity) arises from a completely different mechanism which we'll cover separately in the future.
What makes spasticity distinct?
Two things.
First, spasticity is velocity-dependent. This means that the resistance it produces changes depending on how quickly a muscle is being stretched. Move a limb slowly, and resistance may feel relatively manageable. Move it quickly, and the muscle fights back. The faster the movement, the greater the resistance. That speed-dependent quality is the defining feature.
Second, spasticity originates from exaggerated stretch reflexes — a specific circuit in the nervous system that has lost its ability to stay regulated. So to understand why that matters, we need to look at how that circuit works.
The Reflex Arc
Think back to the last time you touched something unexpectedly hot. Chances are your hand pulled away before you even registered what had happened. That's a reflex — and the automatic nature of it demonstrates something fundamental about how your nervous system is designed.
Your brain is extraordinarily capable, but it takes time to process information and send a response. In situations where speed is critical, waiting for the brain to weigh in could be dangerous. So your nervous system has a shortcut in the form of reflex arcs — fast, automatic circuits that travel only as far as the spinal cord, entirely below the level of conscious thought.
The stretch reflex
The particular reflex relevant to spasticity is the stretch reflex. Unlike the example above that is triggered by heat, this one exists to protect muscles from being overstretched.
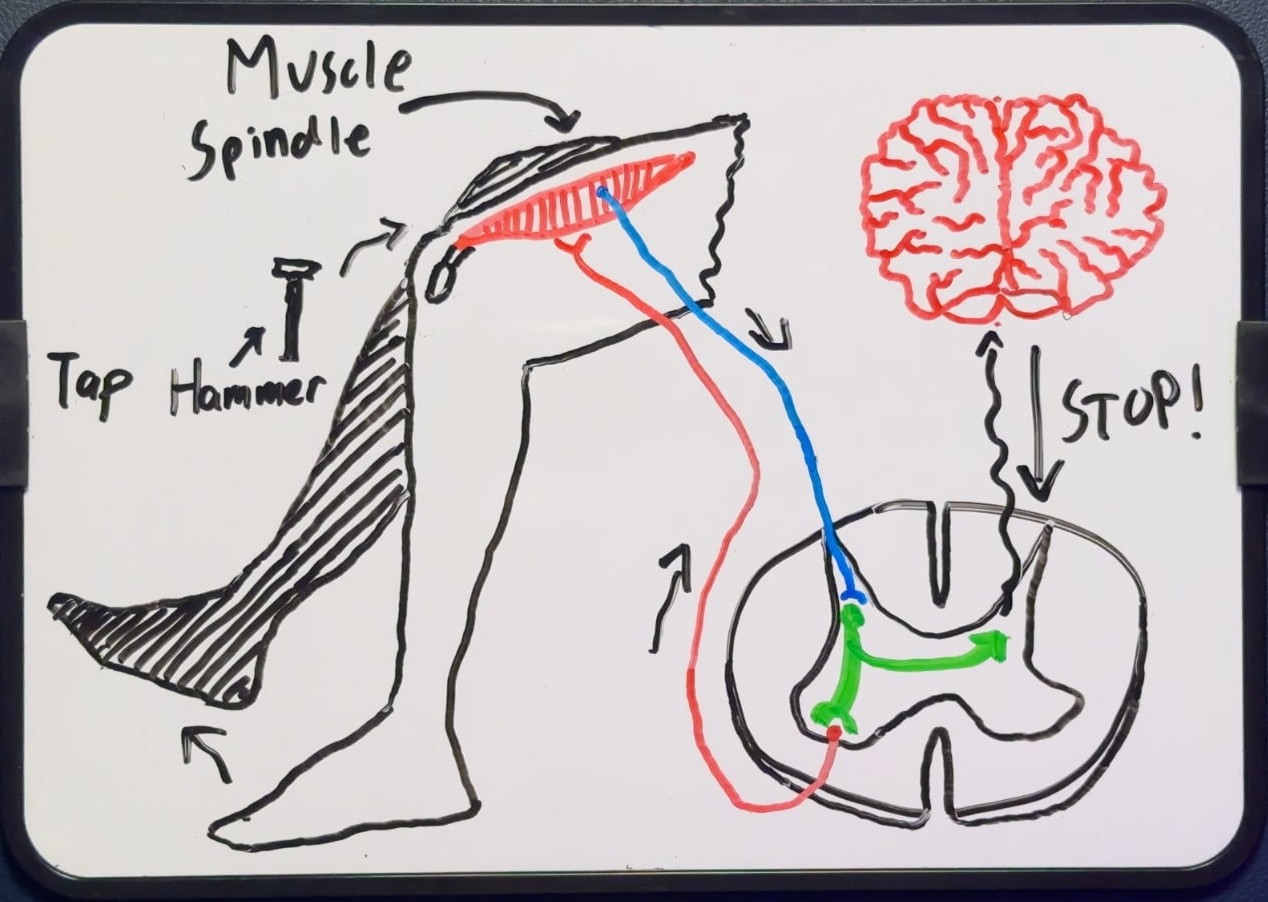
Inside every muscle and tendon are tiny sensory organs — muscle spindles and Golgi tendon organs — that continuously monitor changes in muscle length and tension. When a stretch is detected, these organs send a signal to the spinal cord, which immediately fires back to the same muscle, telling it to contract and resist the stretch.
The classic demonstration is the knee-jerk reflex which you've probably experienced at the doctor's office at some point. A tap on the patellar tendon briefly stretches the quadriceps muscle, causing the spindles to fire, the reflex to activate the quadriceps, and the knee to extend — all without any involvement from the brain.
Descending inhibition — the brain's dial
Stretch reflexes are always present, in every muscle, in every person. Which raises an obvious question — if it's constantly active, why don't muscles fire every time we move?
The answer is descending inhibition.
Your brain is continuously monitoring reflex activity through dedicated pathways in the spinal cord. When it detects reflex activity that isn't needed, it sends inhibitory signals downward, dampening the response at the spinal level through specialised cells called inhibitory interneurons.
Think of the stretch reflex as the ABS in your car — a built-in safety system designed to respond to sudden events. Descending inhibition is like having a sensitivity dial on that system. In a healthy nervous system, the brain keeps that dial at a sensible level. The reflex fires when it's genuinely needed. Otherwise, it stays quiet.
When the Brake Fails
Spasticity occurs when the brain can no longer adequately control that dial.
When the descending brake is damaged — through injury or disease affecting the central nervous system — the reflex arc runs unchecked. Stretch reflexes fire more easily, more strongly, and more persistently than they should. This loss of inhibitory supraspinal control is the defining feature of upper motor neuron syndrome, of which spasticity is a hallmark sign.
It is also remarkably common: spasticity affects approximately 35% of stroke patients, more than 90% of individuals with cerebral palsy, around 40% of those with spinal cord injury, and between 37% and 78% of people with MS. (Winkle, Huang & Lui, NCBI Bookshelf)
However, the way this plays out depends on where the damage occurs.
Stroke
In a stroke affecting the motor cortex, the brain loses its ability to send signals — including inhibitory ones — usually down one side of the body (though this depends on the exact areas of the brain affected). The descending pathways on the affected side are disrupted, and without their brake, the reflex arc on that side becomes hyperexcitable. Because it's typically one hemisphere affected, the spasticity tends to appear on just one side of the body.
Spinal cord injury
In a spinal cord injury, the pathways aren't disrupted at the source — instead they're physically cut off along the way. Everything above the level of injury remains intact. Everything below it loses its descending inhibitory control. This is why someone with a mid-back injury might have full use of their arms but significant spasticity in their legs, while a higher-up neck injury can affect all four limbs.
Multiple sclerosis
In MS, the picture is different again. Rather than one discrete injury, MS causes patchy demyelination — which is damage to the myelin sheath insulating nerve fibres at multiple points throughout the brain and spinal cord. Think of electrical wiring with sections of worn insulation. Signals become slowed, distorted, or intermittently blocked. When this affects the descending inhibitory pathways, the result is an unreliable brake — one that malfunctions sporadically, for different muscles, to different degrees. This is part of why spasticity in MS can fluctuate so unpredictably, worsening with heat, fatigue, or during a relapse.
Despite these differences in location and condition, the core mechanism is always the same: the descending brake is compromised, and the stretch reflex runs without its regulator.
The Different Faces of Spasticity
Spasticity isn't a single, uniform experience. It exists on a spectrum, shaped by how much inhibitory control has been lost and how quickly a muscle is being stretched. Understanding the different forms it can take helps make sense of what you might be experiencing in your own body.
Hypertonia
At the milder end is hypertonia — a persistent, background increase in resting muscle tone (resistance caused by muscle activity). The reflex arc is excitable enough that even slow movement produces some resistance. It isn't dramatic, but it's constant, causing joints to feel heavier and stiffer throughout the day, making activities like dressing, transferring, or simply trying to relax more effortful than they should be.
Catch-and-release (clasp-knife response)
With faster movement and less inhibition, that stiffness becomes sharper. A quick stretch fires the reflex strongly — causing a sudden spike in resistance — before some delayed inhibition allows the tension to slowly release. This is sometimes called a clasp-knife response, and the catch-and-release quality it produces is one of the hallmarks clinicians look for during assessment.
Clonus
With even less inhibition, something more self-sustaining can develop. A quick stretch fires a strong reflex contraction — but that contraction then stretches the opposing muscle, which fires its own reflex, which causes the first muscle to stretch again. This is clonus — rhythmic, involuntary oscillations in a self-sustaining loop. We often see it occur at the ankle, usually triggered by sudden movement like taking a step downstairs. It can last a few beats or much longer, and because it can be provoked during everyday movement, it can become a significant safety concern (e.g., for falls).
Spastic dystonia
Finally, there's a presentation that doesn't follow the same rules as the rest. Spastic dystonia isn't triggered by stretch or movement at all. It's a tonic overactivity at rest — the motor neuron defaulting to a sustained "on" state because descending inhibition is so far gone that even baseline neural activity goes unregulated. The muscle is simply contracted, regardless of position. This often affects multiple muscle groups and can significantly impact whole-body posture and movement, making it one of the more limiting presentations in daily life.
Technicality: It's worth noting that spastic dystonia is distinct from non-spastic dystonia, which arises from a different neurological mechanism entirely. Spasticity and dystonia are phenomenologically and pathophysiologically distinct entities, and spastic dystonia represents a subset of dystonia with pathophysiological mechanisms more in common with spasticity (Lumsden, 2023). We personally like to think of it as a bit of a hybrid between involuntary muscle activity caused by dystonia, combined with heightened reflexes from spasticity.
In practice, these forms rarely appear in isolation. Most people with significant spasticity experience several of them layered together, shifting with fatigue, temperature, activity level, and time of day.
Managing Spasticity — and Why It Can't Wait
Spasticity is uncomfortable and exhausting. It interrupts sleep, complicates movement, and makes straightforward tasks feel anything but. The good news is that help is available — and while the right approach will always depend on your specific condition and goals, there are some well-established principles worth understanding.
Exercise and neuroplasticity
In milder cases, frequent, slow, and sustained stretching is a cornerstone of management, by maintaining flexibility and preserving range of motion. Alongside this, targeted exercise to build strength and motor control around an affected muscle can help the brain begin to rewire through neuroplasticity. The nervous system can gradually develop new strategies to regain control. The descending brake may never work exactly as it did before — but with consistent, appropriate input, it can adapt and begin to re-modulate what's been lost
Medical management
For more severe spasticity, medical management plays an important role. Botulinum toxin (Botox), administered by a doctor, works by blocking the signal between the nerve and the muscle — forcing it to relax. That reduction in tone opens an important treatment window. With the muscle quieter, stretching becomes more effective, and rehabilitation therapies can achieve more than they could when fighting against persistent overactivity.
Early Intervention Prevents Contracture
Whatever form management takes — it needs to be consistent.
When a muscle is persistently overactive and shortened, the body begins to adapt to that position. The tiny contractile units inside muscle fibres — called sarcomeres — are gradually lost. Collagen builds up. The tissue stiffens and physically shortens. This is called contracture.
Once contracture develops, it is often irreversible. The joint can no longer move freely, because the tissue itself has structurally changed around that shortened position.
In adults, this process is serious. Picture someone who has had a stroke and lost use of one arm, which tends to rest curled against their chest. Initially it can be straightened, slowly. But if nothing is addressed over the following months, that window gradually closes — sometimes to the point where attempting to straighten it causes significant pain.
The stakes in children — cerebral palsy
In children, the stakes are higher still. In spastic cerebral palsy, the original brain injury doesn't progress — but its consequences do, because children grow. Bones lengthen. Spastic muscles, already shortened and overactive, can't keep pace with that growth. The mismatch widens year by year, leading to progressive contracture, joint deformity, and functional decline that could have been prevented with early intervention. The younger the child, the faster they are growing, and the more urgently that mismatch needs to be addressed.
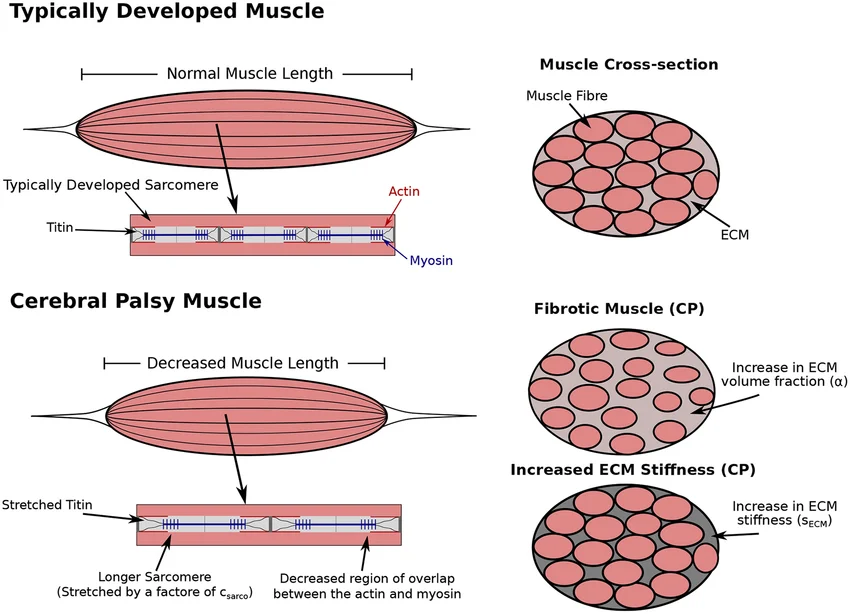
Retrieved from Konno et al., 2022
A Foundation, Not a Destination
Spasticity is a neurological symptom that is complex, individual, and far more nuanced than the label "tight muscles" suggests. But it is also a symptom with a mechanism — one that, once understood, makes the rationale for early and consistent management much clearer. Or so we believe!
That said, if spasticity is significantly affecting your daily life, or if you are a parent navigating this for a child with cerebral palsy, input from a neurologist or neurological physiotherapist is strongly recommended. Early management matters more than most people realise — but now you do. It is considerably easier to prevent contracture from developing than to address it once it has.
And for those looking for structured, condition-specific support to manage spasticity alongside their clinical team, that is exactly what our PhysiKits are designed for (shameless plug 😉)
References
Emos MC, Agarwal S. Neuroanatomy, Upper Motor Neuron Lesion. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-.
https://www.ncbi.nlm.nih.gov/sites/books/NBK537305/
Konno, R. N., Nigam, N., Wakeling, J. M., & Ross, S. A. (2022). The contributions of extracellular matrix and sarcomere properties to passive muscle stiffness in cerebral palsy. Frontiers in Physiology, 12, 804188.
https://doi.org/10.3389/fphys.2021.804188
Lumsden, D. E. (2023). Spastic dystonia: Still a valid term. Developmental Medicine & Child Neurology, 65(10), 1308-1315.
https://doi.org/10.1111/dmcn.15582/
Winkle MJ, Huang D, Lui F. Spasticity. [Updated 2026 Feb 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-.
https://www.ncbi.nlm.nih.gov/books/NBK507869
Stay Informed!
News, updates, and science delivered to your inbox.
We will never sell your information, for any reason.
